
October 2002

A 60-year-old Italian-speaking woman with chronic lymphoblastic
leukemia presents with a 3-day history of fever, chills and hematochezia.
Initially she was seen in the oncology clinic, started on ciprofloxacin
and metronidazole and sent immediately to the emergency. She was
diagnosed with CLL 9 years ago and had received radiotherapy and
various chemotherapy agents. Most recently she received fludarabine
and cyclophosphamide one month ago.
On
examination she had a temperature of 39.4°C with a blood pressure
of 100/70 and heart rate of 120 bpm. The neurologic examination
was normal and she did not have signs of meningismus. There was
marked abdominal lymphadenopathy and prolapsed hemorrhoids that
were most likely the cause of the blood in her stool.
Her
routine blood work was normal. There was no growth from her urine
culture. However, gram-positive bacilli were seen in one out of
two blood culture bottles after one day of incubation. The bacteria
were described as small coccobacilli in short chains. (Figure
1)
The
patient was immediately switched to ampicillin 2g IV q4h and gentamicin
80mg IV q8h. She quickly improved and was stepped down to just
ampicillin for a total of two weeks. Upon further questioning,
it was revealed that in the week prior to her illness she ingested
unpasteurized goat cheese imported from Italy.
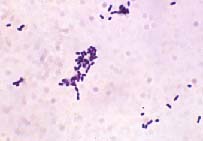
Figure 1: Gram Stain of Isolate reveals gram-positive
bacilli.

- 1. What is the bacterium found in her blood? What diseases
can this bacterium cause?
- Where is this bacterium normally found? How does it cause
disease in humans? Which populations are at most risk? What
advice would you give this patient upon discharge?
- Describe the mechanism of pathogenesis at the cellular and
molecular level.
- How would you confirm the identity of this organism?
- What antibiotics can be used against this bacterium? Which
common antibiotics have no activity against it?

Listeria
monocytogenes is a facultative anaerobic gram-positive rod
that can cause serious infections in humans and animals. While
it is well known as an animal pathogen, L. monocytogenes
is a relatively rare cause of human illness. L. monocytogenes
is ubiquitous in nature as a soil organism and has many opportunities
to enter the human foodchain. The pathogenesis of listeriosis
depends on the ability of the organism to survive and replicate
inside host cells including macrophages. L. monocytogenes
was discovered by Murray, Webb and Swann in 1926 during an outbreak
among lab rabbits and guinea pigs in Cambridge, England. This
new species was originally named Bacterium monocytogenes because
of a profound mononuclear leucocytosis observed in infected animals.
It should be noted that while mononuclear leucocytosis is a characteristic
of some animal infections, it is not a normal feature of human
listeriosis. Other names were also used including Erysipelothrix
and Listerella before Listeria was finally adopted in 1927 to
honor Dr. Joseph Lister, the English surgeon who discovered antisepsis.
L.
monocytogenes primarily causes meningitis, encephalitis and
septicemia especially in the elderly or persons with lower cell-mediated
immunity. It can start with non-sepcific symptoms of fever, malaise
and myalgia or gastrointestinal symptoms before progressing to
a more serious illness such as meningitis in predisposed individuals.
Focal infections are rare but can occur in the immunocompromised
through seeding during the bacteremic phase of the infection.
These include endocarditis, endophthalmitis, septic arthritis,
osteomyelitis, liver abscesses, cholecystitis, peritonitis and
pleuropulmonary infection. Cutaneous infections are also possible
in healthy people who have had skin contact with L. monocytogenes.
In
pregnant women, L. monocytogenes causes a flu-like illness
that can lead to infection of the fetus. Perinatal infections
can lead to abortion, stillbirth or delivery of a seriously ill
baby with early onset listeriosis characterized by pneumonia,
septicemia and disseminated abscesses. Neonatal listeriosis usually
occurs term babies who are infected days to weeks post-delivery
and presents with meningitis rather than septicemia.
While
most cases are sporadic, outbreaks have been documented. Foods
that have been implicated include coleslaw, soft cheeses, pate,
poultry, turkey frankfurters, mushrooms, milk and pork tongue
in jelly. A transient carrier state can occur in 2 to 20% of animals
and humans. Factors that are important in establishing infection
include the host immune status, gastric acidity and inoculum size.
L.
monocytogenes is a facultative intracellular pathogen that
can survive inside host macrophages. It is believed that the bacteria
penetrate the intestinal epithelium through specialized epithelial
cells overlying the Peyer’s patches called M cells. After
invading and replicating in the epithelial and phagocytic cells,
it spreads to the liver and spleen through the bloodstream. Most
are killed in the liver within the first 6 hours. However, if
any bacteria survive, the liver becomes the primary site of replication
for the bacteria. Subsequently they disseminate hematogenously
preferentially to the brain and placenta to cause a more serious
disease. Its ability to survive inside phagocytic cells is thought
to allow entry past the blood-brain barrier and the transplacental
barrier.
L.
monocytogenes is also able to spread from cell to cell without
entering the extracellular environment. To invade host cells,
L. monocytogenes binds to a host receptor called E-cadherin
via a bacterial ligand called internalin. After entry into the
host cell, it resides in a vesicle. Then it must produce a hemolysin
called listeriolysin to lyse the phagosome and escape into the
cytoplasm where it can replicate. Through the expression of a
protein called ActA, it can then harness the host cell’s
actin machinery to move inside the cytoplasm. Upon reaching the
cell membrane, it can cause the pseudopod-like protrusions that
reach out to neighboring cells. Through an unknown mechanism,
the bacterium induces the neighboring cell to engulf the pseudopod
containing the bacterium. It ends up in a second phagosome and
the life cycle is repeated. Thus it can spread from one cell to
the next while avoiding the host humoral immune response.
Listeriae
are gram-positive non-sporulating bacilli or coccobacilli occurring
singly or in short chains. Occasionally palisades and Y-form patterns
can lead to confusion with Corynebacterium. The occasional
rod over 10 µm resembles Erysipelothrix and coccoid
forms can be mistaken for Streptococci. Confirmation
of the identity requires isolation and culture. Colonies are small,
smooth and grayish in color. L. monocytogenes exhibits
tumbling motility at ambient temperatures (20 to 25°C) due
to the presence of up to four peritrichous flagella. It is also
catalase positive, oxidase negative, hydrolyzes esculin, and has
positive Voges-Proskauer and methyl red reactions. L. monocytogenes
produces a hemolysin resulting in β-hemolysis on sheep blood
agar plates. A synergistic hemolysis also occurs with β-lysin-producing
Staphylococcus aureus in the CAMP test. A DNA probe assay
is available for confirmation of colonies on primary plates. Though
not commercially available, PCR-based tests have been shown to
be highly sensitive and specific for detecting L. monocytogenes
in CSF and tissue.
The
pattern of antibiotic susceptibility has remained unchanged for
many years. Penicillin or ampicillin with or without an aminoglycoside
is generally recommended for treatment of listeriosis. Penicillin
alone is bacteriostatic against Listeria but an aminoglycoside
can enhance the activity of penicillin against L. monocytogenes.
Trimethoprim-sulphamethoxazole alone has also been used with success
in listeriosis. Resistance to chloramphenicol, macrolides and
tetracyclines has been reported in some clinical isolates. However,
L. monocytogenes is intrinsically resistant to cephalosporins
and these agents should never be used if Listeria is suspected.

Centers
for Disease Control and Prevention. 2002. Listeriosis. Centers
for Disease Control and Prevention, Atlanta, GA.
http://www.cdc.gov/ncidod/dbmd/diseaseinfo/listeriosis_g.htm
Canadian
Food Inspection Agency. 2001. Food safety facts on Listeria. Ottawa,
Canada.
http://www.inspection.gc.ca/english/corpaffr/foodfacts/listeriae.shtml
Ryser,
E.T. and Marth, E.H. 1999. Listeria, Listeriosis, and Food Safety,
Volume 92. Marcel Dekker, Inc., New York.
|


